We are pleased to present at our Medical Spa the Antibody test for COVID-19. This is not a test to see if you are sick with the virus, but rather to know if you have had it or not. If you have been sick with the virus, but didn’t know it, the result will show antibodies in the blood. Please read the information about the test below. And if you have any questions please call us.
We are happy to try and be part of the solution to the current Pandemic with our Serum antibody C-19 test.
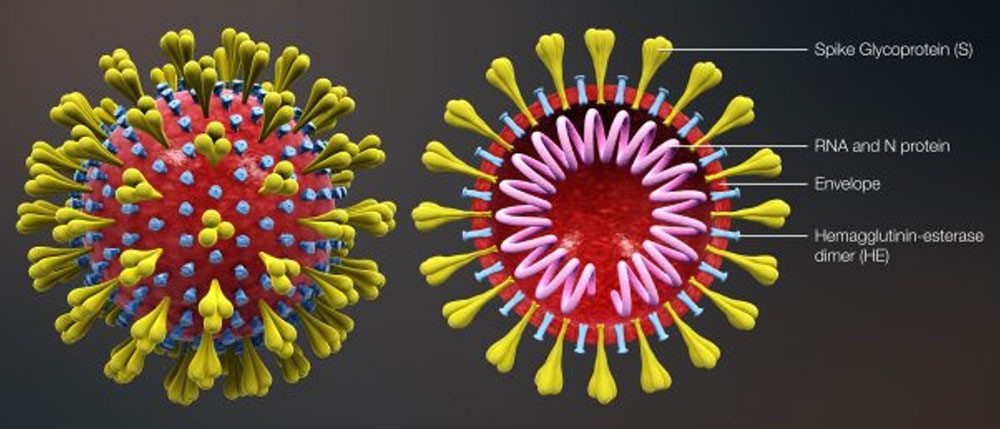
The kit detects 2019-nCoV IgM and IgG antibodies by immuno-capture method. The nitrocellulose membrane is coated by mouse-anti human monoclonal IgM antibodies, mouse-anti human monoclonal IgG antibodies, and goat-anti-mouse IgG antibodies. The recombinant 2019-nCoV antigen and mouse IgG antibodies are labeled with colloidal gold as a tracer. The antibodies will bind to colloidal gold-coated 2019- nCoV antigens to form compounds, which are further captured by pre-coated mouse-anti human IgM antibodies to form new compounds and generate real time results.
Collection Method – COVID-19 Fingerstick Test – FAQ
What is the turn-around time for test results?
The result will be provided back in 48-72
How was the dry blood spot test validated?
Blood from a finger stick was blotted onto filter paper and dried. In parallel, serum from each sample was analyzed. As you can see, there is a 98.84% agreement between Blood Spots and Serum IgM and IgG.
What are the chances of past exposure to coronavirus giving a false positive?
In general, not to common coronaviruses that cause the common cold. The KBMO test measures Nucleoprotein (N) to SARS, SARS-CoV2 (COVID-19) and is very specific for this virus and does not cross react with the common coronaviruses that cause the common cold, sore throat or flu: 229E, HUK-1, OC43 and NL63.
How is this antibody test validated?
This test is validated through clinical trials using real samples of over 2 million tests in China. Three clinical trials summarized as follows:
- Cohort of 447 patients 100% were clinically excluded and tested IgM/G negative. In addition to the usual sensitivity,87.3% 110/126 specificity 100% of 62/62 clinical cases. This test is used in conjunction with a clinical diagnosis and if a person is IgM/G positive the PCR result and other clinical symptoms are considered. A positive IgM/G result would be a presumptive diagnosis that the patient has been infected and should quarantine and be retested at a later date.
- Cohort of 304 clinically diagnosed patients: Class I: PCR + Ab pos: 34.5% by PCR and of these IgM/G picked up 96%, Class II PCR Neg+Ab Pos 41.4% IgM/G pos 41.4% so Antibody picked up 74% of pos and PCR only 34.5%.
- FUO 73/304 Cohort 202 pts healthy or had fever, IgM-G testing picked up 99% of clinically confirmed cases.
Sensitivity, specificity, False Positives and Test Timing?
IgM/G shows 100 and 99% specificity. False positives are ruled out clinically. For example, 24% of patients showed fever that was not related to COVID-19 and were PCR/IgM/G negative and it was determined clinically that fever of unknown origin (FUO) due to another cause.
False positive is a clinical determination not a test per se. Cohort of 202 patients: 99% of clinical positives were correctly predicted by IgM/G testing.
False negative is the most important parameter because the person is free to spread the virus.
This test will pick up 96% of PCR positive and 74% of all positives whereas PCR picks up only 34.5% of clinically positive patients.
Please remember that it takes a few days to be PCR positive (prodromal phase) and then a few days longer for IgM/IgG to show. Tests are just a snapshot in time and if you test in the wrong window you could be infected and be PCR or Ab negative. So, you can get a false negative if you miss the window. It takes about 28 days for most people to seroconvert to IgG. So, the test result is dependent the timing of the sample. Also, PCR which is the gold standard only picks up 34% of confirmed positive patients whereas, antibody testing picks up 41%.
- IgM-G/PCR negative: the person is not infected, FUO?
- PCR positive/Antibody negative: infection
- IgM-G pos/PCR negative: infection
What Ig classes are represented by the IgG band
The anti-human IgG in this test will detect: IgG1/2/3/4. IgG3 is a strong activator of complement and will promote viral clearance via the liver and spleen via CR1.
What are the interfering factors?
IVIG Rx would most likely result in a positive IgG test but less likely to be IgM positive because convalescent plasma is mostly IgG and would be used which contains high titer of IgG neutralizing antibodies.
Many different coronaviruses and related viruses or even bacterial antibodies do not cross react with the test antigen NP, antivirals do not interfere, heparin/EDTA/Citrate do not interfere, and non-specific IgM/G does not interfere. Icteric, hyperlipemia and hemolyzed samples may interfere.
What about mutations and the different strains of COVID-19? Will this test detect them?
There are 6 strains are circulating, and most mutations are in the S1 domain of the spike (RBD).
If you have had COVID-19 and recovered or were asymptomatic, how long will you have IgG antibodies?
Antibodies to Coronaviruses have been shown to be present for 12 years. Post infection and generation of IgG generally indicates immunity. There are some exceptions.
Do you know if we still must be quarantined UNTIL we have results of this test?
If you have been exposed to a known infected person quarantine is advised for at least 7-14 days even after testing negative. It takes a few days to be PCR positive (prodromal phase) and then a few days longer for IgM/IgG to show. Tests are just a snapshot in time and if you test in the wrong window you could be infected and be PCR or Ab negative. So, you can get a false negative if you miss the window. It takes about 28 days for most people to test positive for IgG.
Would you recommend this test to establish immunity especially for health care workers, those who suspect exposure or need to confirm immunity?
This test will indicate who was infected but does not indicate immunity. However, in the IgG positive convalescent phase many different antibodies are being produced against a lot of different viral proteins: N, M, E and S. Antibodies against the S protein RBD domain that inhibits binding to the host ACE2 receptor block viral entry and play a role in neutralizing the virus. Neutralizing antibodies are measured in a separate assay that shows convalescent plasma blocks virus binding to cells and prevents plaque formation.
What does the presence of antibodies tell us about possibility of reinfection vs. protection? What do we know at this point?
What we know is that the production of a robust IgG response is essential to generate immunity. Re-infection is always possible but the ability to mount a rapid IgG response is essential to block subsequent infection. As new strains emerge, re-infection with a different strain is always possible, and in this case, one would have to mount a new IgM and IgG response all over again.
How valid is the test for patients who congenitally or have an acquired low total serum IgG and/or IgM levels?
There are cases where certain patients may be immunodeficient either genetically, through a disease process or another co-morbidity. Even in these cases, if one is exposed or infected it still would be a clinically valuable tool.
*Please remember that testing is an aid to diagnosis and provides evidence but cannot be used in exclusion.
Call our spa today!!!
-
Solea Medical Spa and Beauty Lounge your first and final destination for all your beauty and medical needs.
info@soleabeautylounge.com